Society for Psychotherapy Research Annual Meeting · Osaka, 2026
Last month I had the privilege of presenting at the Society for Psychotherapy Research international conference in Osaka — three contributions that together amount to the clearest statement I have been able to make of a research programme I have been building for many years. I want to share the main threads here, because they feel more timely now than ever.
The Problem We Are Not Quite Naming
Psychotherapy research has become very good at demonstrating that treatments work. It has become less good at explaining why they work — and, critically, for whom and when. The dominant model remains one of symptoms, clusters, and manualised protocols: you identify a disorder, you apply the corresponding treatment, you measure whether the symptoms decrease. The model is clean, it satisfies funders and regulators, and it has delivered real improvements in population outcomes.
But something important is left out. Clinicians know this. They encounter people whose symptom profiles fit no clean diagnostic category, whose responses to standard treatments are partial or unstable, and whose most pressing problem is not what they feel or do, but a pervasive loss of flexibility — an inability to move, to shift, to recover from disruption.
What if that inflexibility is not a secondary feature of the disorder, but its defining characteristic?
Symptoms as Attractors
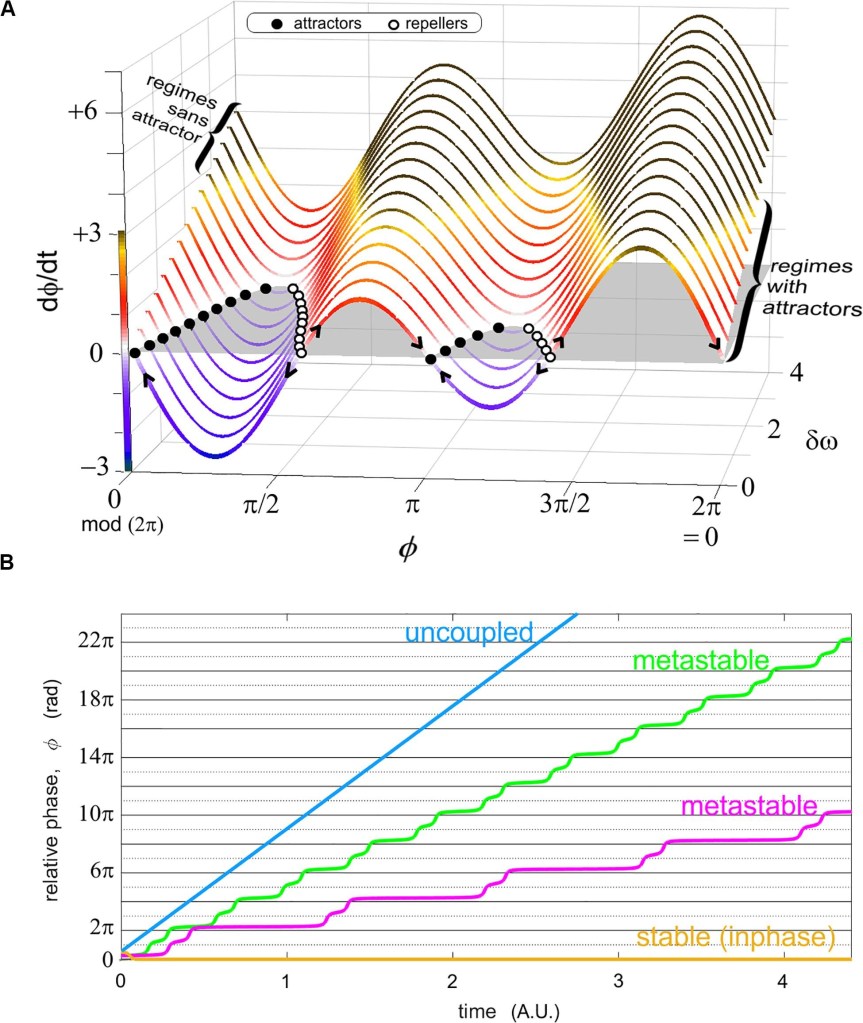
Complexity science has a vocabulary for this. In dynamical systems terms, the states we call symptoms may be better understood as attractors — stable configurations that the system falls into and finds difficult to leave. The question changes: we are no longer asking how to suppress a state, but how to reshape the landscape within which states are possible. Treatment, on this view, is the work of restoring the system’s capacity to move.
Two central concepts run through all three of my Osaka presentations.
Coordination is the broad term: the lawful patterning of coupled parts, from neural firing to interpersonal interaction. Synchronization is the specific case of phase-locking — when the rhythms of two or more systems become temporally coupled. These are not metaphors. They are measurable, with tools that already exist: heart rate variability (HRV) analysis, EEG phase synchrony, Recurrence Quantification Analysis (RQA), the Kuramoto order parameter across oscillator networks.
The clinical intuition that follows from this is simple but consequential: health looks like metastable re-coordination, not maximal synchrony. Rigid locking — the state in which a system cannot decouple — is not health. It is a trap. What we want, both in the nervous system and in the therapeutic relationship, is the capacity to synchronize, to desynchronize, and to find a new configuration — repeatedly, across timescales.
What We Mean When We Say “Synchrony”
One thing I tried to do in the structured discussion that opened our panel was to slow the conversation down around the word synchrony, which has become genuinely slippery in the field. A synchrony claim is actually empty unless six dimensions are specified: the modality of what is being coupled (motor, physiological, affective, linguistic); the directionality (who drives whom); the phase sign (matching or complementary — turn-taking is anti-phase synchrony, not the absence of synchrony); the timescale of the measurement window; the flexibility of the coupling; and the level of inference (are we measuring co-occurrence, or can we claim coupling as a mechanism?).
The recurring error in the literature — and in the clinic — is using one method while asserting another. A researcher might measure co-occurrence of movement and claim interpersonal coupling. The measures do not license the claim without appropriate controls (surrogate testing; a directional analysis method). Getting this right matters not just for publications but for clinical thinking. If we are trying to intervene on synchronization dynamics, we need to be clear about which aspect of synchronization we are actually targeting.
From Phenotypes to Treatment
The most clinically developed work I presented concerns Complex Emotional Needs — the population of young people (16–25) whose difficulties span emotional dysregulation, interpersonal coordination failures, and a pervasive instability that resists categorical diagnosis. These are people for whom standard protocols frequently fail, not because the protocols are poorly designed but because the protocols are not designed for them.
Working with colleagues at the Norfolk and Suffolk NHS Foundation Trust and the University of Amsterdam, I have been developing a framework that reconceptualises CEN as a multi-scale coordination disorder — with dysregulation manifesting across autonomic, affective, and interpersonal timescales simultaneously. Rather than a symptom profile, each person has a coordination landscape that can be characterised by four parameters derived from attractor topology: curvature (κ), energy barrier (ΔE), Lyapunov exponent (λ), and noise amplitude (σ).
From this landscape analysis, four coordination phenotypes emerge:
- Hypervigilant: rigid over-synchronization, narrow and deep attractor basin, hyperactivated autonomic nervous system, enmeshed interpersonal coupling
- Collapsed: reduced synchronization, flat landscape, affective numbing, social disengagement
- Chaotic: unstable coordination, fragmented attractors, rapid dysregulation with poor recovery
- Balanced: flexible synchrony, moderate basin depth, high HRV complexity, adaptive proximity-autonomy cycling
These phenotypes are not four new diagnostic categories. They are descriptions of the current state of a landscape — a landscape that can and does shift across a treatment episode. The clinical implication is that intervention should be matched to the landscape, not to the symptom cluster.
IDEAS: A Dynamical Systems Treatment
The IDEAS programme (Interventive Dynamic Emotion Assessment and Skills) is an 8-week group-based treatment for young people with CEN, structured around four modules that each address a specific synchronization domain: interpersonal coordination (Connect, Communicate, Coordinate); autonomic regulation (Distress Tolerance); affective coordination (Emotion Regulation); and action-environment coupling (Behavioural Flexibility). Modules are weighted adaptively based on initial phenotype assessment and session-by-session monitoring — not assigned rigidly by diagnosis.
Preliminary data from a pilot study of 48 participants show large effect sizes (Cohen’s d > 0.8) across outcome domains, with improvements maintained at three-month follow-up. Crucially, phenotype-stratified analyses confirm differential trajectories: HRV complexity increases across all groups; metastability indices shift toward the balanced range; Hypervigilant phenotypes show the greatest reduction in autonomic rigidity, Collapsed phenotypes the greatest increase in interpersonal engagement, and Chaotic phenotypes the greatest reduction in coordination entropy.
These findings are preliminary and replication is needed. But they suggest that the theoretical architecture is pointing in a useful direction: that the right unit of clinical prediction is not the diagnostic category but the coordination phenotype.
Rupture, Repair, and Phase Transitions
I want to close with what is perhaps the most familiar clinical phenomenon — rupture and repair — reinterpreted through this lens. Every therapeutic relationship involves moments of misattunement, disengagement, or breakdown. Standard relational models describe rupture-repair cycles as opportunities for growth and mentalisation. Dynamical systems theory adds something: these are also phase transitions.
At the moment of rupture, we can expect to see measurable physiological signatures — critical slowing down, loss of metastability, the system approaching a bifurcation point. Repair is not a return to the prior state; it is the emergence of a new coordination state, with an expanded attractor landscape and enhanced resilience. This reframing changes what therapists are watching for, and what they are trying to do when they repair.
What Comes Next
Three implications seem most urgent to me.
For research, we need multi-level coordination measurement built into standard process-outcome designs. HRV, EEG synchrony, and RQA are feasible in clinical settings; what’s been missing is the theoretical framework to make their results interpretable. That framework is now available.
For treatment development, the Coordination Balancing Algorithm (CBA) provides a decision-support architecture for adaptive modular treatment — selecting and reweighting intervention modules based on landscape topology rather than symptom presentation. This is the logic that IDEAS operationalises, and that I hope to extend to other populations.
For training, the ask is genuinely new: therapists need dynamical literacy — the ability to read coordination signatures in session and calibrate their responses to the landscape features they observe. This is not a replacement for relational skill; it is a complement to it.
An AI-assisted coordination monitoring tool (IDEAS Coach) is in development. I will write more about that separately.
Franco Orsucci is a researcher and clinician at the Norfolk and Suffolk NHS Foundation Trust and the University of Amsterdam. He is also a founding member of the Mind Force Society — mindforce.foundation.